
For many adults, the right time to get a first bone health assessment is earlier than current standard guidelines suggest. If you have risk factors, a family history of osteoporosis, or have recently gone through menopause, waiting until age 65 may mean missing a critical window. .
This guide walks through everything that determines your personal testing timeline — so you can make a clear, confident decision about your bone health today.
What Is a Bone Density Test and Why Timing Matters
A bone density test is an assessment of how strong and dense your bones are. It detects low bone mass before fractures occur, which is what makes early timing so valuable.
The challenge is that bones weaken gradually over years, and by the time a fracture happens, significant loss has often already occurred. Getting assessed at the right time is where prevention actually starts.
| What It Measures | Why It Matters | What It Can Prevent |
| Bone mineral density (BMD) | Shows how much mineral is packed into your bones | Identifies risk before fractures occur |
| Bone quality and microstructure (REMS only) | Reveals the internal architecture of bone tissue | Detects deterioration that density scores alone miss |
| Fracture risk score | Combines density and quality data for real-world risk | Guides proactive lifestyle and nutrition decisions |
| Rate of bone change over time | Tracks whether bone health is improving or declining | Measures impact of nutrition, exercise, and supplements |
Bone Density vs. Bone Quality
Strong bones are not just about density. Two people with the same bone density score can have very different fracture risk depending on bone quality.
Compared to the standard DXA scans which measure only the density, REMS (Radiofrequency Echographic Multi-Spectrometry) assesses both density and quality, which is why it provides a more complete picture of actual fracture risk.
Why Bone Loss Has No Early Symptoms
Bones do not hurt as they weaken. This is the core problem with relying on symptoms alone. Most people discover they have osteoporosis only after a fracture, often from a minor fall that a healthy bone would have survived easily.
By the time back pain, height loss, or stooped posture appear, bone loss is typically already significant. That is why proactive assessment is the more effective approach.
Recommended Ages for Bone Density Testing
The Columbia University Irving Medical Center, recommends that women start bone density screening at age 65 and men at age 70. These are reasonable starting points for the general population, but they are not strict rules.
Bone loss accelerates significantly during perimenopause and early menopause, which typically begins in the mid-40s to early 50s. Waiting until 65 means missing a decade or more of the most critical monitoring window.
| Group | Standard Guideline Age | Recommended Starting Age (Proactive) | Why |
| Women (general) | 65 | 40-50 (at perimenopause) | Rapid bone loss begins during hormonal transition |
| Women (with risk factors) | Earlier than 65 | 35-45 | Family history, low weight, or early menopause accelerates loss |
| Men (general) | 70 | 50-60 | Gradual loss accelerates after 65 without early baseline |
| Men (with risk factors) | Earlier than 70 | 45-55 | Steroid use, low testosterone, smoking, or low BMI increase risk |
| Athletes / active adults | Any age | 20-30 for baseline | RED-S, overtraining, and low body weight affect bone health early |
| Young adults (especially if have risk factors like) with restricted diets while growing up | N/A | 30 | Young adults who followed restricted diets should be screened around the age of peak bone density to assess their bone health and future risk. |
| Pregnant women | N/A | During pregnancy or while breastfeeding/lactation | Pregnant or breastfeeding women can develop temporary osteoporosis, especially with low BMI or other risk factors, and should be screened if needed. |
Women: Why Screening Often Starts Earlier
Estrogen in women plays a major protective role in bone health. When estrogen levels fall during perimenopause and menopause, bone loss speeds up significantly. Some women lose a notable portion of their bone mass in the years around menopause.
Getting a baseline assessment before this hormonal shift — ideally in your early 40s — gives you a reference point that makes future monitoring far more meaningful. You cannot track change without knowing where you started.
For women already in or past menopause who have not yet had a bone assessment, starting as soon as possible is the right move. Understanding how to prevent osteoporosis starts with knowing your current bone status.
Men: Later Screening but Not Lower Risk
Men lose bone more gradually than women and are significantly under-screened as a result. The assumption that osteoporosis is a women’s condition leads many men to skip assessment entirely — sometimes until after a fracture.
Male osteoporotic fractures, particularly hip fractures, are associated with serious outcomes. Although osteoporotic fractures occur more frequently in women, men who sustain hip fractures experience higher post-fracture mortality rates than women with the same injury, highlighting the severe consequences of osteoporosis in men.
Testosterone decline after 65 accelerates bone loss in men. A baseline scan in the early 50s gives a useful reference for tracking change through that transition.

You May Need a Bone Density Test Earlier If You Have These Risk Factors
Age alone does not determine when you need a bone density test. Several medical, lifestyle, and genetic factors accelerate bone loss and move the ideal assessment timeline earlier — sometimes by a decade or more.
| Risk Factor | Why It Increases Risk | Consider a Bone Health Assessment By |
| Early menopause (before 45) | Earlier loss of estrogen protection means longer period of accelerated bone loss | Age 40 or at time of menopause |
| Long-term corticosteroid use | Steroids reduce calcium absorption and suppress bone-forming cells | Within 6 months of starting steroid therapy |
| Family history of osteoporosis or hip fracture | Genetics account for a significant portion of bone density variation | Age 40 for women, 50 for men |
| Low body weight or underweight BMI | Less mechanical load on bones reduces density; lower estrogen in low-weight women | Age 35 to 40 |
| Previous fracture from low-force impact | A fragility fracture is a direct signal of already-compromised bone strength | Immediately after the fracture |
| Thyroid or parathyroid disorders | Hormonal imbalances directly affect bone turnover and mineral metabolism | At time of assessment |
| Chronic malabsorption conditions (e.g., celiac, Crohn’s) | Impaired nutrient absorption affects calcium and vitamin D uptake | At time of assessment or shortly after |
| History of eating disorders | Low calorie intake and nutrient deficiency during key bone-building years have lasting effects | Age 30 to 35 |
Medical Conditions and Medications
Several common medications interfere with bone metabolism when taken long-term. Corticosteroids are the most widely recognised, but proton pump inhibitors, certain diabetes medications, and hormone-blocking cancer therapies also carry bone health implications.
Cancer Treatments That Significantly Affect Bone Density:
Breast Cancer Therapies:
- Aromatase inhibitors such as anastrozole (Arimidex), letrozole (Femara), and exemestane (Aromasin) cause 4-5% bone loss over 2 years and increase fracture risk by 35-50%
- GnRH analogs (gonadotropin-releasing hormone agonists) used in premenopausal women
- Chemotherapy drugs including doxorubicin and cyclophosphamide, which can induce early menopause
- Oophorectomy (surgical removal of ovaries), causing immediate estrogen loss
Prostate Cancer Therapies:
- Androgen deprivation therapy (ADT) reduces bone mass by 4-5% per year
- GnRH agonists and antagonists
- Androgen receptor inhibitors
Other Medications:
- Proton pump inhibitors (long-term use for acid reflux)
- Certain diabetes medications
- Long-term corticosteroid use (prednisone, cortisone)
Clinical guidelines recommend baseline and annual bone density monitoring for all patients starting aromatase inhibitor therapy or androgen deprivation therapy.
If you are on long-term medication in any of these categories, a proactive bone assessment is worth discussing with your healthcare provider.
Lifestyle Factors That Accelerate Bone Loss
According to the National Library of Medicine, smoking can reduce bone mass and increase fracture risk. Heavy alcohol use has been associated with reduced bone mass and increased fracture risk. They both should be avoided for a variety of health reasons.
A sedentary lifestyle removes the mechanical load that stimulates bone maintenance. Bones respond to physical demand — without it, bone turnover slows and density declines faster.
Low calcium and vitamin D intake over time compounds these effects. Bones draw on stored minerals when dietary intake falls short, gradually depleting the bone matrix.
Family History and Genetics
If a parent has had osteoporosis or a hip fracture, your own risk is meaningfully higher. Genetics influence peak bone mass, bone turnover rates, and the pace of age-related decline.
A family history alone is sufficient reason to pursue a bone health assessment before standard screening ages, regardless of how healthy your lifestyle is.
Similarly, having a small frame or low BMI alone is sufficient reason for earlier assessment, as lower body weight reduces mechanical load on bones and is associated with lower bone density.
A Simple Self-Check: Do You Need a Bone Density Test Now?
Use this quick decision matrix to assess your personal situation. If more than two items in the left column apply to you, a bone health assessment is worth prioritising now rather than waiting for a standard guideline age.
| If this describes you… | Consider a bone health assessment… |
| Women aged 40 or older approaching perimenopause or menopause | Now, do not wait for the standard age guideline |
| Man aged 55 or older with any additional risk factor | Within the next 6 to 12 months |
| You have had a fracture from a low-force impact at any age | As soon as possible — this is a direct warning sign |
| You have taken corticosteroids for 3 or more months | At the time of or shortly after starting therapy |
| You have a parent who had a hip fracture or osteoporosis | By age 40 to 45 for women, 50 for men |
| You are an athlete with low body weight or irregular periods | Now — RED-S and low energy availability affect bone health at any age |
| You feel fine and have no symptoms | Still worth considering — bone loss has no symptoms until fracture occurs |
Quick Yes or No: Is It Time for Your Bone Health Assessment?
Ask yourself these questions. Each ‘yes’ adds weight to the case for getting assessed sooner rather than later.
- Are you a woman aged 40 or older?
- Have you gone through or are you approaching menopause?
- Do you have a parent who had a hip fracture or osteoporosis?
- Have you ever broken a bone from a minor fall or low-force impact?
- Do you smoke, or have you smoked regularly in the past?
- Have you taken steroid medication for three or more months?
- Do you have a thyroid condition, celiac disease, or another chronic condition affecting absorption?
- Are you a man aged 55 or older?
Three or more ‘yes’ answers puts you in a category where proactive assessment is genuinely worth prioritizing now.
Special Situations That Change Your Testing Timeline
Certain life events and health conditions shift your bone density test timeline significantly. These are not rare edge cases, they affect a large portion of adults in their 40s, 50s, and 60s.
| Situation | Impact on Bone Health | Recommended Timing Adjustment |
| Menopause before age 45 | Accelerated bone loss for longer period | Get a baseline assessment at time of menopause |
| Surgical menopause (oophorectomy) | Immediate, sharp drop in estrogen and bone protection | Assessment within 6 months of surgery |
| Fragility fracture after age 40 | Indicates bone strength may already be compromised | Immediate assessment after fracture |
| Chronic corticosteroid therapy | Ongoing suppression of bone-forming activity | Within 6 months of starting; annual monitoring thereafter |
| Assessment of celiac or Crohn’s disease | Impaired mineral absorption over time | At or shortly after assessment |
| Athlete with low energy availability (RED-S) | Bone stress without adequate nutritional support | Assessment as soon as RED-S is suspected |
| Recent significant weight loss | Reduced mechanical load on bones; possible nutritional gaps | Within 6 to 12 months of significant loss |
Menopause and Hormonal Changes
Menopause is the single biggest turning point for bone health in women. The hormonal shift accelerates bone turnover and tips the balance toward net bone loss. For most women, the most rapid decline happens in the first few years after menopause.
Getting a bone health assessment at or just before this transition gives you an accurate baseline. From there, regular monitoring shows whether bone health is holding steady or requires attention.
Previous Fractures After Age 40
A fracture from a low-force impact (a fall from standing height, bumping a table, or a minor stumble) is not a normal outcome for someone with healthy bones. It is an important early signal that bone strength may already be reduced.
If this has happened to you, it is one of the strongest individual indicators for getting a bone density assessment, regardless of age.
Athletes and Highly Active Individuals
High activity levels do not automatically mean strong bones. Athletes with low body weight, restricted calorie intake, or irregular menstrual cycles are at risk of a condition called Relative Energy Deficiency in Sport (RED-S), which impairs bone formation.
Endurance athletes, dancers, and gymnasts are among the groups most commonly affected. A bone health assessment gives a clear picture of whether training and nutrition are supporting or working against bone strength.
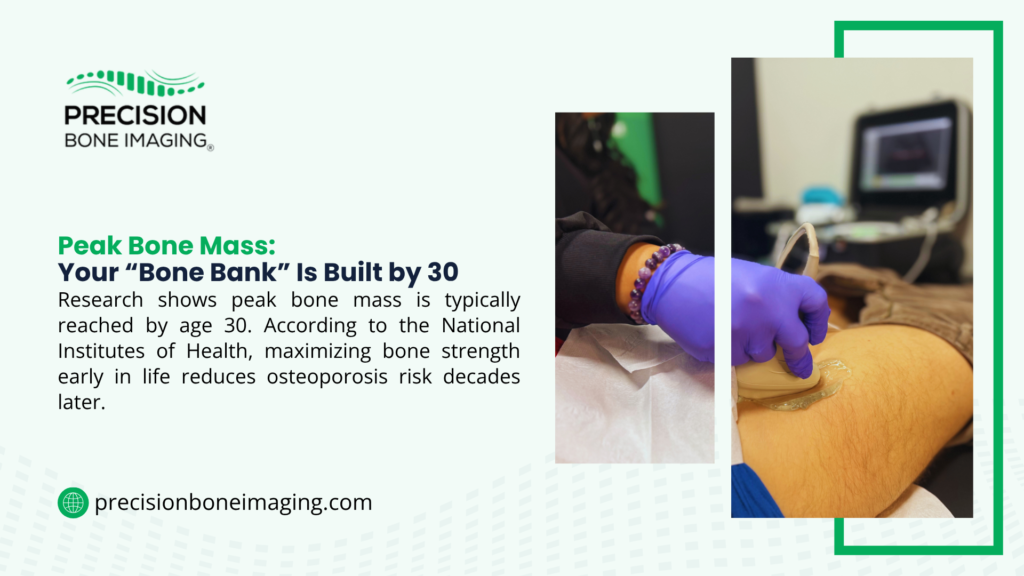
What Happens During a Bone Density Test?
One of the most common reasons people delay bone health assessments is simple uncertainty about the process. The experience is straightforward, non-invasive, and takes very little time.
With REMS technology, no radiation is involved at any point. The assessment uses ultrasound-based echographic multi-sensor technology applied at the hip or lumbar spine, and results are available immediately.
| Step | What Happens | How Long |
| Arrival and check-in | Brief health history review and confirmation of assessment site | 5 minutes |
| Positioning | You lie or sit comfortably while the sensor is placed at the hip or spine | 2 to 3 minutes |
| Assessment | REMS technology scans the bone site using radiation-free ultrasound sensors | 5 to 10 minutes |
| Results review | Instant results are reviewed on-screen including density, quality, and fracture risk score | 5 minutes |
| Guidance summary | You receive a clear summary of your findings and recommended next steps | 5 to 10 minutes |
Is the Test Painful or Dangerous?
A REMS assessment involves no pain, no radiation, and no preparation beyond comfortable clothing. Unlike a standard DXA scan, there is no X-ray exposure — making it safe for repeat assessments over a lifetime and suitable for anyone from age 20 upwards.
REMS is FDA-registered and CE-marked. The technology is unaffected by arthritis, scoliosis, or metal implants, which makes it accessible for a broader range of individuals than standard DXA scanning.
How to Prepare for Your Bone Health Assessment
Preparation for a REMS assessment is minimal. The main steps are:
- Wear comfortable, loose-fitting clothing — no metal fasteners near the hip or lower back
- Bring any previous bone scan results if you have them — they help establish a baseline for comparison
- Avoid eating or drinking for 2-3 hours before your appointment to minimize abdominal gas that may interfere with lumbar spine imaging
How Often Should You Repeat a Bone Density Test?
A single assessment gives you a snapshot. The real value of bone health monitoring comes from tracking whether your bones are responding to lifestyle changes, nutrition, or supplements.
REMS is radiation-free, which means repeat assessments carry no cumulative exposure risk. This makes it practical to monitor at intervals that would not be advisable with X-ray-based scanning.
Additionally, REMS assesses the inner trabecular bone structure where bone remodeling begins, rather than just measuring overall density like DXA.
This means REMS can detect meaningful changes in bone quality in as little as 6 months, significantly faster than traditional density-only scans.”
If you want to understand more about how to increase bone density through lifestyle changes, regular monitoring is the only reliable way to know if what you are doing is working.
| Result Category | Typical Retest Interval | Notes |
| Normal bone density, low risk | Every 2 to 3 years | More frequent if lifestyle changes or new risk factors emerge |
| Osteopenia (low bone mass) | Every 12 to 18 months | Track response to nutrition, exercise, and supplementation |
| Osteoporosis findings | Every 6 to 12 months | Monitor closely; consult with healthcare provider on next steps |
| Post-fracture monitoring | Every 6 months initially | Higher frequency until bone status stabilises |
| Active lifestyle intervention | Every 6 to 12 months | Useful to confirm whether changes are producing measurable results |
Monitoring the Progress of Your Bone Health
One of the most motivating aspects of regular bone health monitoring is seeing results. When nutrition, resistance training, and supplementation are working, repeat assessments show measurable improvement in both density and quality scores.
This is particularly true with REMS, which tracks bone quality changes that a standard density-only scan would miss.
A modest change in density may come alongside a more significant improvement in bone quality, something that only shows up in a more detailed assessment and REMS can detect these changes in as little as six months.

What to Do After Your Results: Normal, Low, or Osteoporosis
Results from a bone density assessment fall into one of three categories. Each one has a clear set of next steps, and none of them require immediate alarm — they require action.
| Result | What It Means | Next Steps |
| Normal bone density | Your bone strength is within a healthy range for your age | Maintain nutrition and exercise habits; retest in 2 to 3 years |
| Low bone mass (osteopenia) | Bone density is lower than optimal but not yet at osteoporosis level | Review calcium, vitamin D, and protein intake; add resistance training; retest in 12 to 18 months |
| Osteoporosis findings | Significant reduction in bone strength; fracture risk is elevated | Consult your healthcare provider; focus on fall prevention, nutrition, and load-bearing exercise |
| Elevated fracture risk score | Risk score indicates increased vulnerability even with moderate density | Proactive lifestyle review with guidance from your provider; more frequent monitoring |
Improving Bone Health at Any Age
Whatever your results, bone health responds to consistent effort. The main pillars are resistance exercise, adequate calcium and vitamin D, sufficient protein, and avoiding the lifestyle factors that accelerate bone loss.
Bones are living tissue, and they adapt to the demands placed on them. Bone Density Scan Cost and Insurance is a common concern that stops people from getting assessed, but understanding your actual out-of-pocket options often removes that barrier faster than expected.
Age is not a limiting factor for bone improvement. Studies show measurable gains are achievable into the 70s and 80s with the right combination of exercise and nutrition.
FAQs: When Should You Get a Bone Density Test?
At what age should I get my first bone density test?
For women, a baseline assessment around age 40 to 45 is valuable before the hormonal changes of perimenopause accelerate bone loss. For men, a baseline in the early to mid-50s provides a useful reference point. Standard guidelines recommend age 65 for women and 70 for men, but these are minimum thresholds, not optimal ones.
Do I need a bone density test if I have no symptoms?
Yes. Bone loss has no symptoms until a fracture occurs. That is precisely why proactive assessment matters. Waiting for a sign that something is wrong means the window for early prevention has already passed.
What risk factors mean I should test earlier?
Early menopause, a family history of osteoporosis or hip fracture, long-term steroid use, a previous fragility fracture, low body weight, smoking, pregnancy or breastfeeding, or a chronic condition affecting nutrient absorption all indicate earlier assessment. Any two or more of these factors together make earlier testing a clear priority.
How do I know if I am at risk for osteoporosis?
The most reliable way to know is a bone health assessment. Risk factors give an indication, but they do not replace measured data. A REMS assessment provides both bone density and bone quality results, giving you a more complete picture of your actual fracture risk than a standard scan.
Key Takeaway
Knowing when you should get a bone density test is one of the most practical steps you can take for long-term health. The answer is earlier than most people expect and for a significant number of adults, that time is now.
Bone loss is silent, gradual, and preventable when detected early. A proactive bone health assessment gives you clear findings, a fracture risk score, and the information you need to take action — before a fracture does it for you.
Book Your Radiation-Free Bone Health Assessment
At Precision Bone Imaging, we use REMS technology to provide a complete picture of your bone health without any radiation exposure. Results are instant, the process takes around 15 minutes, and you leave with clear, actionable findings.
Having served more than 4,000 people, we are now recognized as a reliable source for early osteoporosis screening and continuous bone health assessment.
Whether you are building a baseline, monitoring change, or following up after a concerning result, we are here to help.Book your radiation-free bone health assessment today and take the first clear step toward stronger bones for life.
